Automatically locating organs in CT images
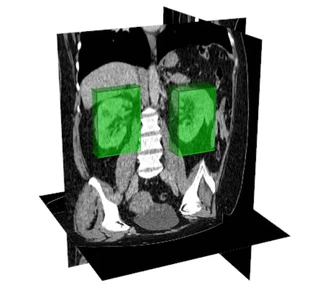 Automatic localization of the kidneys in a CT volume, using bounding boxes
Automatic localization of the kidneys in a CT volume, using bounding boxesMy first turn toward machine learning — taken, with this student, two years before the deep-learning boom.
In the continuation of the LPR project, I co-supervised with Emmanuel Promayon the PhD of Prasad Samarakoon, defended on 30 September 2016 at Université Grenoble Alpes (funded by the French ANR TecSan project “Robacus”). This is the project that tipped me toward machine learning applied to medical imaging. We started two years before the rise of deep-learning segmentation: so we bet not on deep neural networks, but on decision-tree forests (random forests) — a clear-eyed choice for the time, and a formative one.
What this thesis really gave me was not one more method: it was an early familiarity with the strengths and the limits of learning-based approaches — first among them their surprising robustness.
The challenge: locating, not segmenting
To plan a puncture assisted by the LPR robot, one must first locate, in the CT scan, the target organs and those to avoid — a step still done by hand by the clinician, tedious and costly in expert time. Rather than aiming straight for full segmentation (delineating every contour), we tackled the more tractable and equally useful problem of localization: enclosing each organ in a bounding box, automatically.
The contribution
Beyond a thorough analysis of the method, the thesis produced two contributions of real practical reach:
- the Light Random Regression Forests: a faster and far more memory-efficient model, at equivalent accuracy — and therefore easier to embed and deploy;
- an automatic parametrization that removes settings previously fixed “by hand”, making the method more robust and more reproducible from one dataset to another.
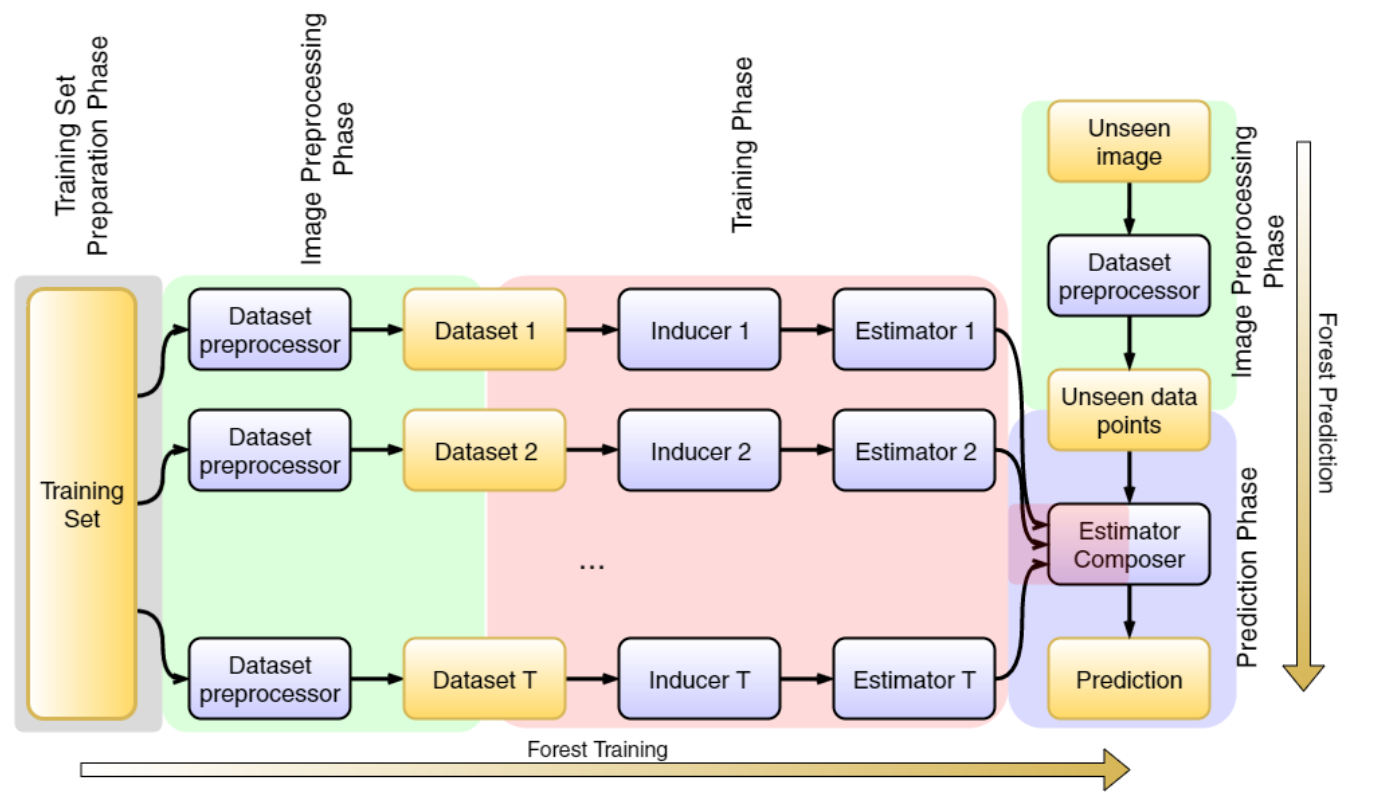
The regression-forest pipeline: training-set preparation, preprocessing, training, then prediction (data in yellow, algorithmic steps in blue)
Robustness — and bias: the phantom-kidney story
One experiment remains, for me, the perfect illustration of what these methods really are. To learn to locate the kidneys, our training database — built from experts’ manual delineations (ours and those of the team’s PhD students) — contained only patients with two kidneys. During the testing phase, the radiologist handed us the image of a patient who had only one. The algorithm dutifully found… two bounding boxes, placing a “phantom kidney” exactly where statistics expected it.
Even then, we were alert to a truth that has lost none of its relevance: a model is only the reflection of the data it is shown. The quality and representativeness of the training set matter as much as the algorithm itself.
What this project represented
With the rise of deep learning, this forest-based localization strategy was later set aside — but it was decisive. It let me approach the machine-learning turn from the foundations, at a time when one still took the time to understand why a method works, what it guarantees, and where it fails. That perspective — robustness, generalization, vigilance about the data — is exactly what I bring today to medical-application prototyping.
Skills involved: doctoral co-supervision · machine learning applied to medical imaging · design of robust, automatic methods · building and critically assessing training datasets.
Related publications
- 2017. Samarakoon Prasad N, Promayon Emmanuel, Fouard Céline — Light Random Regression Forests for automatic multi-organ localization in CT images. 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017)
- 2014. Saramakoon Prasad, Promayon Emmanuel, Fouard Céline — Fully Automatic Organ Localization in Medical Images Using Improved Random Regression Forests. Proceedings of Surgetica 2014
