REMI — Decision Support for Lower-Limb Endovascular Revascularization
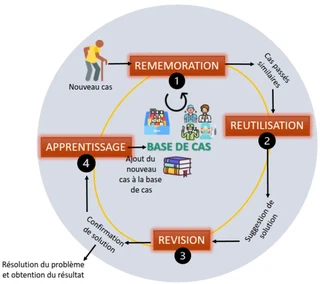 The Case-Based Reasoning (CBR) cycle applied to surgical decision-making (fig. 2.5, M. Roux thesis)
The Case-Based Reasoning (CBR) cycle applied to surgical decision-making (fig. 2.5, M. Roux thesis)How do you help a vascular surgeon choose the best revascularization strategy, when the success of a technique remains hard to predict? REMI explores one answer: learning from past cases — the way an experienced clinician does — but in a tooled, traceable and interpretable way.
The result, first
REMI (from the French Revascularisation Endovasculaire des Membres Inférieurs — Lower-Limb Endovascular Revascularization) is a clinical decision-support project I have coordinated since 2021, in close collaboration with the vascular surgery department of Grenoble Alpes University Hospital. Within a few years, it has made it possible to:
- design and deploy in the clinic a user-centred data-collection software;
- turn real clinical data — incomplete and heterogeneous — into a usable case base;
- demonstrate the relevance of case-based reasoning to suggest, for a new patient, the strategies that succeeded in similar patients;
- bring a doctoral thesis to completion (Margaux Roux, defended with distinction on 16 December 2025) and lead a multidisciplinary team funded by five successive grants.
This project consisted of taking a concrete clinical need, translating it into specifications, removing the technical and organizational roadblocks, and going all the way to a genuinely used prototype.
The clinical problem: a decision that is hard to anticipate
Peripheral Arterial Disease (PAD) of the lower limbs is an arterial condition whose main symptoms are pain and ischemic wounds. To avoid severe complications — amputation, death — revascularization aims to restore blood flow, either endovascularly (angioplasty, stenting) or through open surgery.
The problem: the probability of success or failure of a given technique remains hard to predict. The surgeon relies on decision trees, scores (WIfI) and, above all, on experience. To date, no tool fully helps them choose, for this patient, the most promising strategy.
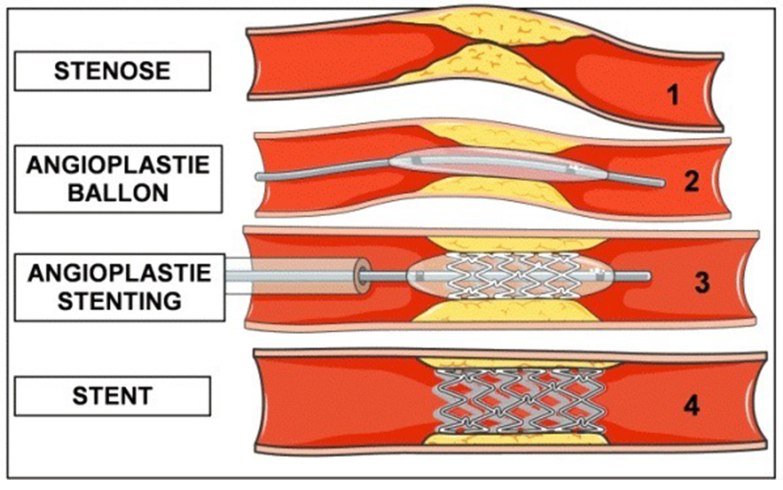
Endovascular revascularization techniques: angioplasty and stenting (fig. 1.9, M. Roux thesis).
A method: case-based reasoning
Clinical decision-support systems traditionally fall into two families: statistical approaches, powerful but often poorly interpretable (“black boxes”), and expert-rule approaches, transparent but hard to scale.
REMI explores a middle path: Case-Based Reasoning (CBR). Its assumption — “similar problems have similar solutions” — translates, in the clinic, into: similar symptoms, treated with similar therapies, lead to similar outcomes. It is a learning method close to medical reasoning itself, and naturally more explainable: every recommendation rests on real cases that can be examined.
The CBR cycle unfolds in four steps (shown in the cover image): retrieve similar cases, reuse and adapt their solution, revise the outcome, then retain the new case to enrich the base.
From raw clinical data to a usable case base
This is often the most underestimated — and most structuring — step. The data available in electronic health records are incomplete, heterogeneous and designed for care, not for analysis. The project therefore had to:
- model a “case”: a set of attributes describing the problem (severity, WIfI score, lesion anatomy, comorbidities) and a second set describing the surgical solution and its outcome;
- explicitly handle missing data and attribute typing;
- combine retrospective and prospective data, then develop a Python extraction-and-aggregation pipeline that transforms patient-centred data into a decision-support-oriented case base.
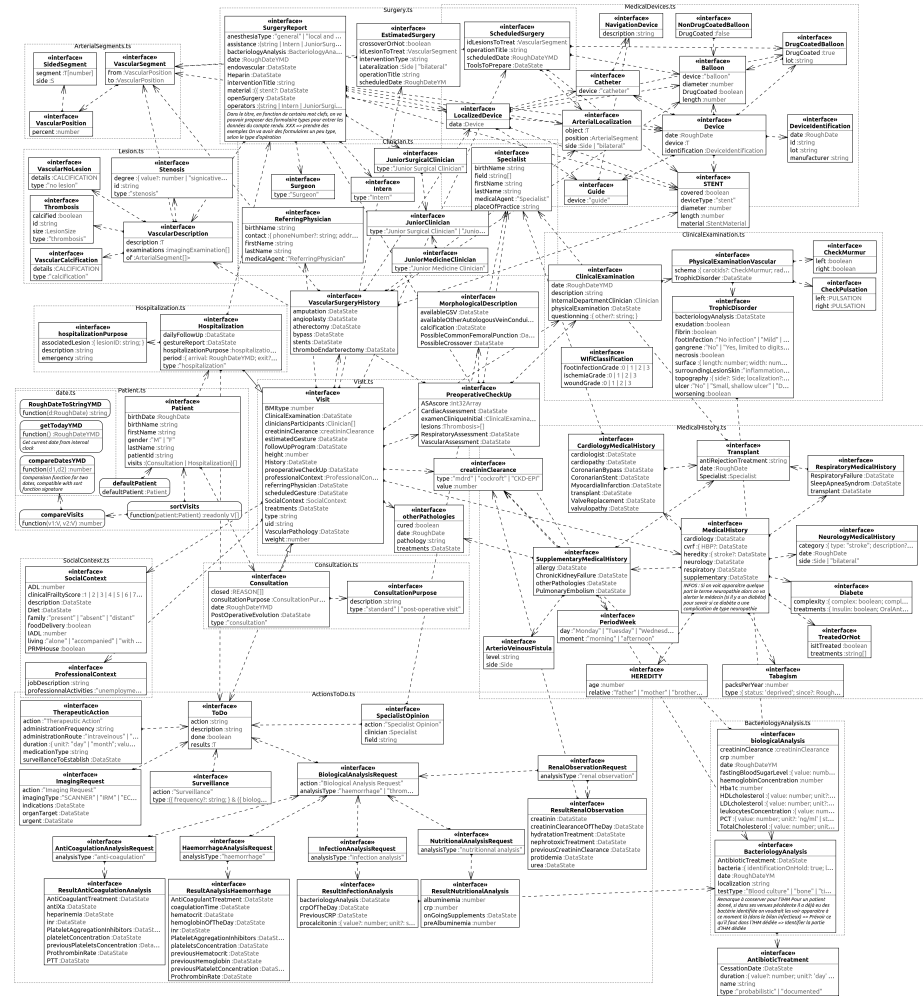
Class diagram of the data model implemented in the collection software (fig. 3.9, M. Roux thesis).
A user-centred prototype, deployed in the clinic
To collect high-quality prospective data, we designed a prototype software directly usable by clinicians, within their workflow. It automatically computes the WIfI score (and thus the amputation risk), models an operation as a sequence of surgical gestures applied to lesions, and automatically generates an operative report.
This is exactly the kind of deliverable I care about: a tool designed with and for its users, robust enough to leave the lab bench and enter clinical practice. Developing this application justified hiring a dedicated research engineer.
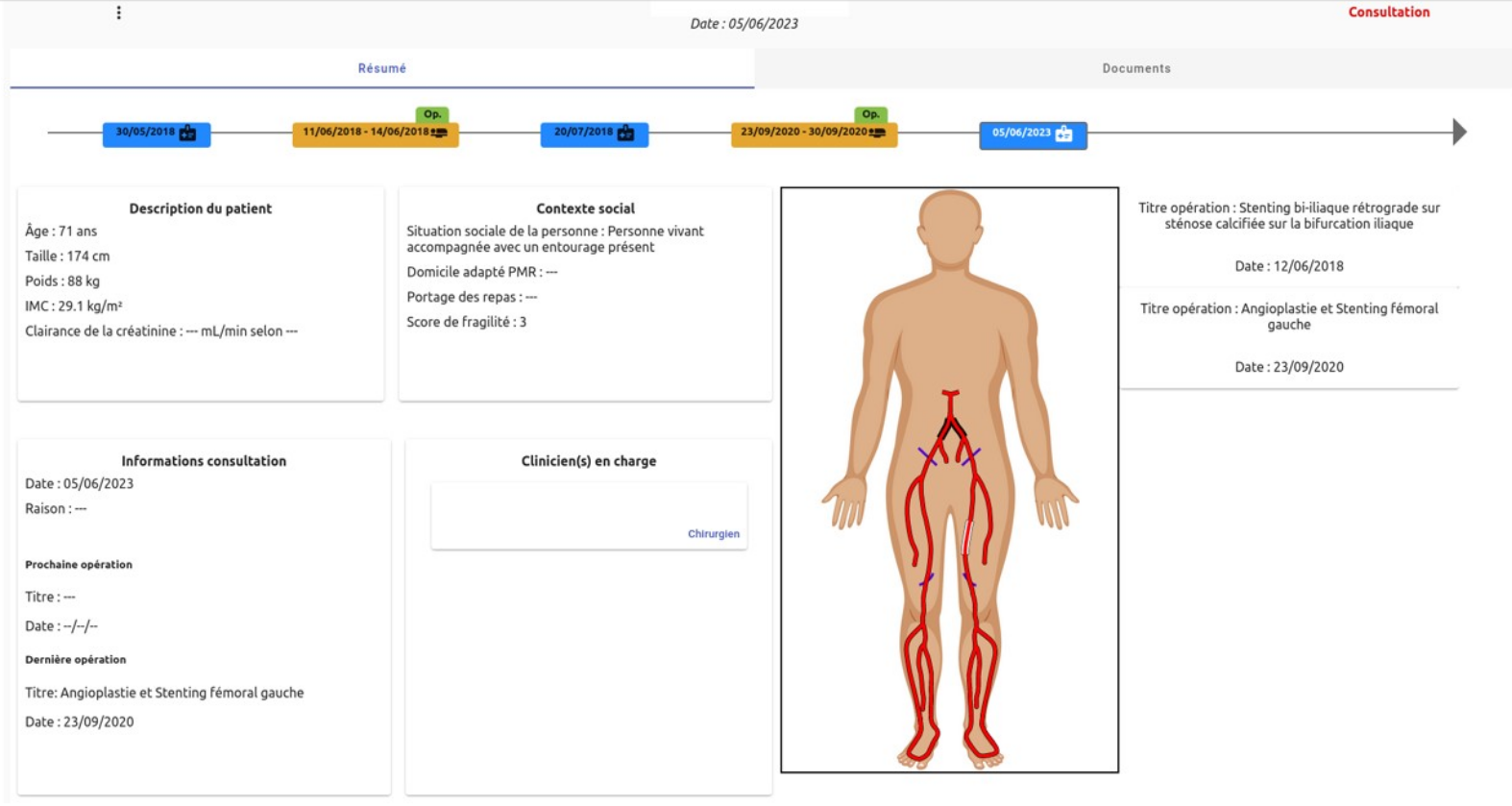
Interface of the prototype data-collection software (fig. 3.11, M. Roux thesis).
Demo video of the software, presented at the project’s first conference (in French).
Representing cases to compare them
Comparing two patients requires a sound similarity measure between cases. The project relies on an autoencoder: a neural network that learns to represent each case in a compact latent space, where geometric proximity reflects clinical similarity. Retrieval of relevant cases then takes place in that space.
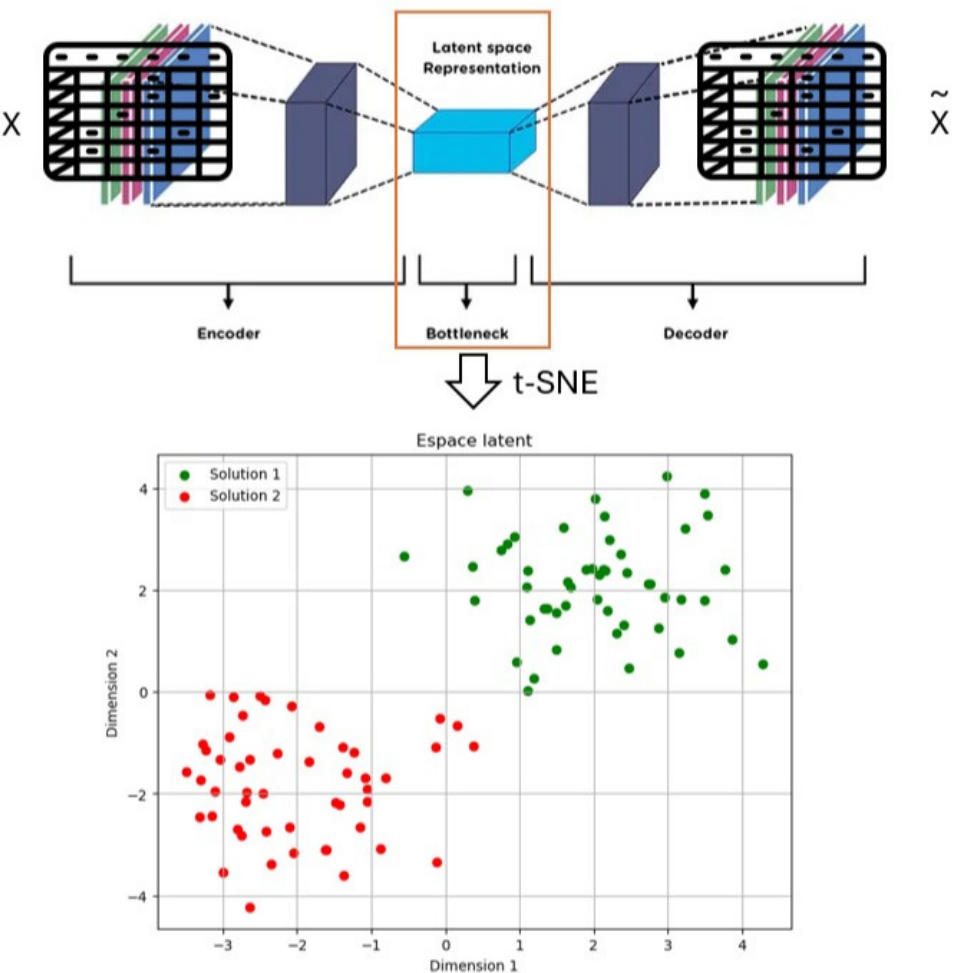
Retrieval of similar cases in the learned latent space (fig. 4.4, M. Roux thesis).
Project leadership and funding
Started in 2021 with Prof. Rafaëlle Spear, the project gradually brought together three sites (TIMC in Grenoble, LTSI in Rennes, Grenoble Alpes University Hospital) and was supported by €284,450 raised from four funding sources.
| Period | Project / scheme | Co-lead(s) | Funding obtained | Source | Amount |
|---|---|---|---|---|---|
| 2021–2022 | REMI-ORIA | Rafaëlle Spear | Equipment | EMERGENCE (TIMC laboratory) | €12,000 |
| 2022–2023 | User-centered development for data collection in endovascular revascularization | Rafaëlle Spear & Alexandre Demeure | 2 Master’s (M2) interns (Laure Chatenet & Clément Gasse) | MIAI@Grenoble Alpes (ANR-19-P3IA-0003) | €11,200 |
| 2024–2025 | CAMI-assistant chair | Sandrine Voros | 1 research engineer for one year (Romaric Ruga) + equipment | MIAI@Grenoble Alpes (ANR-19-P3IA-0003) | €66,056 |
| 2024–2026 | Decision support — REMI | Rafaëlle Spear & Pascal Haigron | 1 PhD student (Margaux Roux) | LabeX CAMI | €160,000 |
| 2026–2027 | Clinical deployment and validation of an AI tool | Rafaëlle Spear | Thesis completion + 1 intern + software subcontracting | Fondation pour l’Avenir | €35,194 |
| Total | €284,450 |
Supervision and collaborations
- Margaux Roux, PhD student — thesis “Decision support for lower-limb endovascular revascularization”, defended on 16 December 2025 (co-supervision at 33% with R. Spear and P. Haigron).
- Laure Chatenet and Clément Gasse, Master’s (M2) interns.
- Romaric Ruga, research engineer (finalizing the data-collection software).
- Prof. Rafaëlle Spear (PU-PH, vascular surgery, Grenoble Alpes University Hospital) — clinical co-lead since the project’s inception.
- Prof. Pascal Haigron (University of Rennes, LTSI) — thesis co-supervisor.
- Sandrine Voros (TIMC) and Alexandre Demeure — co-leads on funding schemes.
Publications
- 2025. Roux Margaux, Spear Rafaëlle, Fouard Céline, Haigron Pascal — Retrieving similar cases for clinical decision support in the context of revascularization of lower limbs. International Journal of Medical Informatics, Vol 201, pp105931
- 2024. Roux Margaux, Spear Rafaëlle, Haigron Pascal, Demeure Alexandre, Fouard Céline — Toward Decision Support System for Lower Limb Endovascular Revascularization. 2024 46th Annual International Conference of the IEEE Engineering in Medicine and Biology Society
- 2023. Spear Rafaëlle, Fouard Céline, Demeure Alexandre, Gasse Clément, Chatenet Laure — User-centered design for the development of a patient monitoring software for peripheral arterial disease. Annals of Vascular Surgery
Together with Prasad Samarakoon’s thesis, this project anchors my work in AI applied to healthcare — with one constant requirement: interpretable methods, genuinely usable tools, and an ongoing dialogue with clinicians.
