Medical Image Analysis
 Transperineal ultrasound-guided implantation — prostate brachytherapy
Transperineal ultrasound-guided implantation — prostate brachytherapyWhen I joined the GMCAO research group at TIMC laboratory in 2006, I contributed my expertise in medical image processing and analysis to three ongoing applied projects led by my colleagues. These collaborations allowed me to tackle diverse clinical challenges — from real-time surgical vision to oncological dose computation — while immersing myself in the tools and culture of the team.
These three projects are grounded in rigorous academic knowledge production: each contribution led to publications in international peer-reviewed journals and conferences, or to a patent filing. The skills described here were forged alongside that scientific output — they are its direct product.
These three projects embody a conviction that has shaped my entire approach: a medical image is only as good as its usability by the clinician, at the right moment and in the right context.
Prostate Brachytherapy — Orientation of Iodine-125 Seeds
Project led by Jocelyne Troccaz (TIMC-GMCAO)
Co-supervision of post-doctoral researcher Giao Nguyen (50%, with Jocelyne Troccaz)
Context
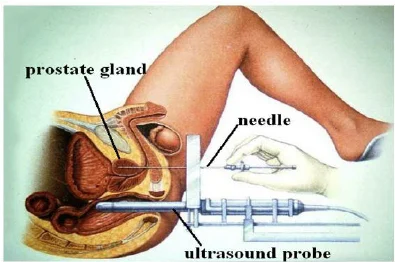
Transperineal implantation guided by ultrasound — clinical context
Prostate brachytherapy involves implanting radioactive iodine-125 seeds directly into the prostate gland. Calculating the radiation dose absorbed by tumour tissue — dosimetry — is critical for evaluating treatment effectiveness and anticipating side effects. At the time, dosimetry tools modelled seeds as isotropic point sources, ignoring their actual orientation within the tissue.
The research question: does seed orientation influence dosimetry enough to warrant its inclusion in clinical software?
Contributions
To answer this, we first needed to automatically detect and localise seeds in post-operative CT images — a challenging task, as seeds are small, closely spaced, and may overlap in projection.
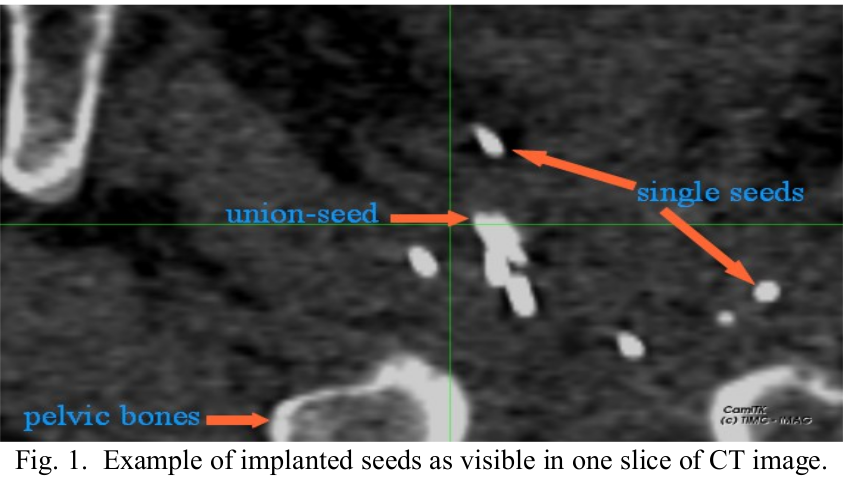
Implanted seeds as visible in a CT slice: single seeds, clustered seeds, and pelvic bones
We developed a complete pipeline for:
- Segmentation of iodine seeds in CT images
- Separation of seeds that touch or overlap
- Pose estimation (3D position + orientation) of each individual seed
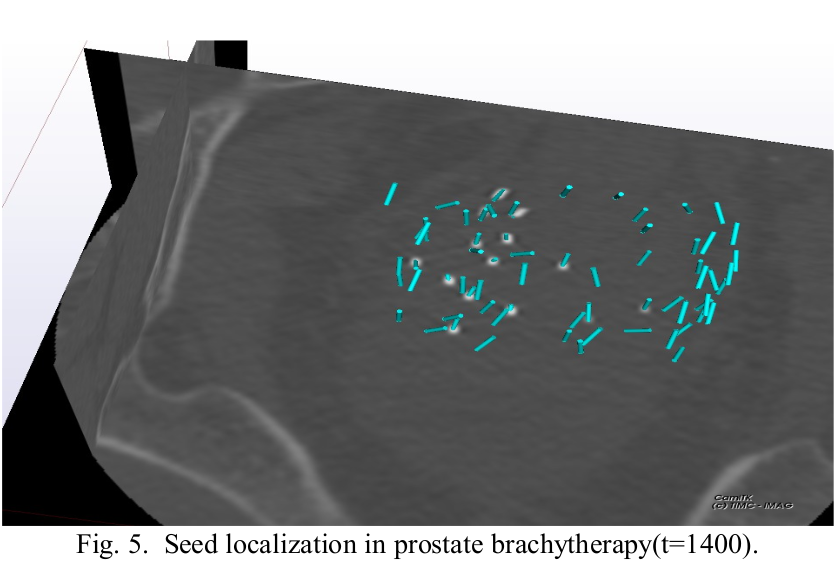
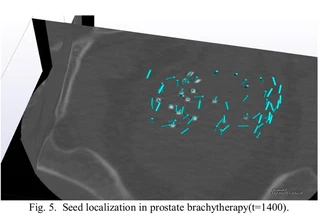
3D localisation of brachytherapy seeds in the prostate (CamiTK visualisation)
Results confirmed that seed orientation had a measurable impact on dosimetry — a clinically significant finding for post-operative evaluation and treatment follow-up.
Skills Applied
- 3D medical image processing (CT)
- Geometric modelling of radioactive sources
- Software development and integration into the CamiTK platform for clinical use
- Validation protocols on real patient data
Related Publications
- [IEEE TBME 2015] H.-G. Nguyen, C. Fouard, J. Troccaz — Segmentation, separation and pose estimation of prostate brachytherapy seeds in CT images — read
- [Cancer/Radiothérapie 2014] F. Meneu, H. Nguyen, C. Fouard et al. — Impact de l’orientation des grains iode 125 dans l’évaluation de la dosimétrie à 1 mois — read
- [Physica Medica 2013] F. Meneu, G. Nguyen et al. — Consideration of seeds orientation in prostate brachytherapy and dosimetry analysis — read
3D Ultrasound-Based Bone Tracking
Co-supervision at 50%, with Jocelyne Troccaz
PhD thesis of Jonathan Schers (2006–2009)
Ultrasound-guided orthopaedic intervention: the clinical context
Context
Orthopaedic procedures — prosthesis placement, osteotomies — require real-time tracking of bone structures during surgery. Classical techniques rely either on X-ray imaging (radiation) or on invasive bone markers. The goal of this project was to explore a minimally invasive alternative: tracking bone structures using 3D ultrasound.
Contributions
We proposed a per-operative tracking method based on 3D/3D ultrasound image registration: from a reference volume acquired at the start of the procedure, bone displacements are tracked by registering each new acquisition against that reference.
Segmentation of the bone surface in an ultrasound image
Key scientific contributions:
- Segmentation of bone surfaces in ultrasound images (noisy signal, reflection artefacts)
- Rigid and deformable registration methods adapted to the ultrasound modality
- Panoramic reconstruction from multiple partial acquisitions
- Evaluation on cadaveric anatomical specimens
Skills Applied
- Ultrasound signal processing
- Multimodal medical image registration
- Design of a ground-truth-free registration validation method
- Doctoral co-supervision (50%)
Related Publications
- [IUS 1007] J. Schers, J. Troccaz, V. Daanen, C. Fouard, C. Plaskos, P. Kilian - 3D/4D ultrasound registration of bone - read
- [IJCARS 2009] J. Schers, J. Troccaz, C. Fouard, C. Plaskos, O. Palombi — 3D/3D ultrasound registration for panoramic volume reconstruction — read
- [CAOS 2010] J. Schers, C. Fouard, J. Troccaz — Non invasive ultrasound-based bone tracking — read
Distributed Laparoscopy — Extended View of the Surgical Field
Co-supervision at 50%, with Philippe Cinquin
PhD thesis of Christophe Boschet (2007–2010)

Standard laparoscopy: a single camera, a narrow field of view
Context
During a laparoscopic procedure, the surgeon’s field of view is very narrow: the endoscopic camera, inserted through a trocar, only covers a small portion of the abdominal cavity. The surgeon must constantly reposition the camera to explore the operative field, which is cognitively demanding and lengthens procedures.
The idea: replace a single high-resolution camera with several small, distributed miniature cameras (similar to the phone cameras of the day), and reconstruct a real-time 3D panoramic view of the operative zone.
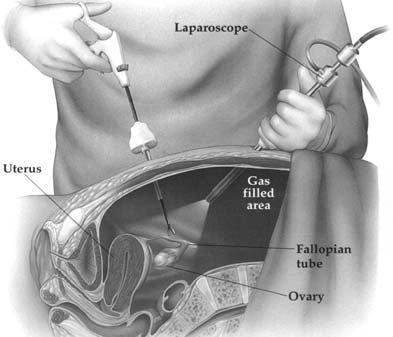
Standard laparoscopy: a single camera, a narrow field of view
Contributions
This project posed novel challenges at the intersection of computer vision and embedded computing:
- Calibration of multiple miniature cameras in an endoscopic configuration
- 3D reconstruction of the surgical field via distributed stereovision
- Fusion of video streams to produce a coherent augmented view
- Integration into the CamiTK platform and prototyping for pre-clinical experimentation
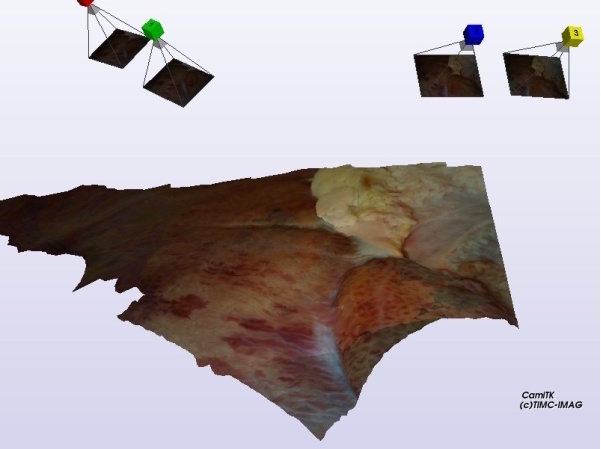
3D reconstruction of the operative field from multiple cameras (CamiTK)
The project remained at the research prototype stage but led to a European patent filing.
Skills Applied
- Stereoscopic computer vision
- Multi-camera optical system calibration
- Hardware/software integration
- Patent writing
Related Output
- [Patent EP 2016] P. Cinquin, S. Voros, C. Boschet, C. Fouard, A. Moreau-Gaudry — Imaging system for the three dimensional observation of an operation field — read
What These Projects Taught Me
These three collaborations were a practical school in medical prototyping — and far more than a checklist of technical skills.
I learned to work with real, imperfect clinical data, often without ground truth available to validate the algorithms. I developed the reflex of designing rigorous evaluation protocols where standard benchmarks didn’t exist, and of integrating operating room constraints from the design phase — time pressure, sterility requirements, ergonomics for the surgeon.
I also shaped my collaborative approach: learning to ask the right questions to clinicians, to translate a medical need into an algorithmic problem, to deliver tools integrated into a software platform usable by non-computer-scientists.
These skills — built alongside a sustained effort in scientific publication and formal knowledge production — are the ones I bring today to medical application prototyping.
