Interventional cardiology
 Image-guided interventional cardiology
Image-guided interventional cardiologyFrom clinical need to prototype: guiding the gesture at the heart of the cath lab.
Interventional cardiology is performed under imaging, yet the clinician must often act without directly seeing the target: the lesion to treat or to biopsy does not appear on the real-time image in the room. Carried out with Prof. Gilles Barone-Rochette (Grenoble Alpes University Hospital) and the LTSI laboratory in Rennes, this project pursues a single goal expressed through two clinical questions: to give the cardiologist reliable guidance, built from preoperative imaging and usable directly in the room.
The common thread: bouncing back when the data runs short
The project started with the guidance of cell therapy. The first clinical trial enrolled fewer patients than expected: the data needed for the next steps were not there. Rather than abandoning it, we redeployed the technical building blocks already developed (image segmentation, navigation) toward a related clinical need with more immediate value and a better-identified bottleneck: endomyocardial biopsy.
This pivot is, in itself, a deliverable: it illustrates the ability to de-risk a project, preserve the assets already built, and refocus the effort where the clinical value is highest — exactly the kind of trade-off a company expects when an R&D programme does not go as planned.
Sub-project 1 — Guiding post-infarction cell therapy
After a heart attack, some therapies consist in re-injecting cells into the myocardium. The whole challenge is precision: reaching the right areas, relying on information (the extent of fibrosis, the viable regions) that is only visible on preoperative imaging, not on the real-time image in the room.
Our approach: fuse multimodal imaging to transfer, during the intervention, the targets identified preoperatively. The core building block is the automatic segmentation of the myocardium and fibrosis on late gadolinium enhancement MRI (LGE-MRI), developed using deep learning as part of Erwan Lecesne’s PhD (co-supervised with the LTSI in Rennes), then integrated into CamiTK to be presented to the clinician in the room.
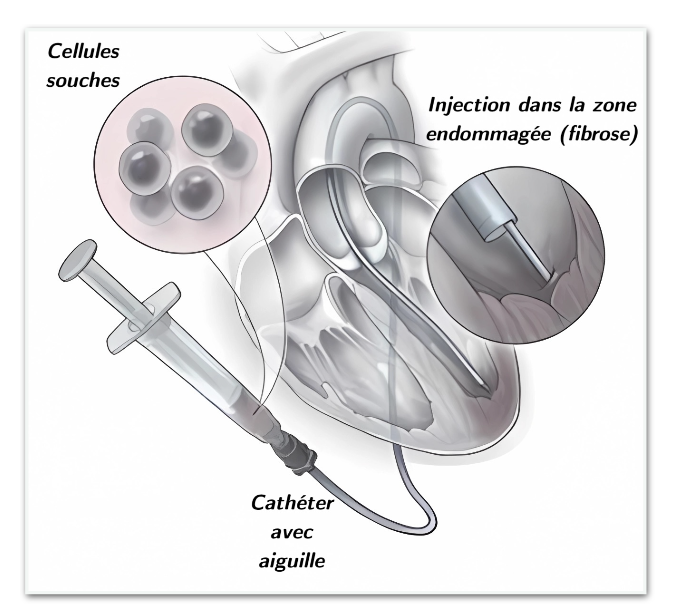
Re-injecting cells in the right place: the precision of the gesture determines the therapy’s effectiveness.
CamiTK is a prototyping toolkit: it makes it possible to move quickly from concept to evaluated prototype, but its output is not meant to be a CE-marked medical device. This building block is therefore a proof of concept; its industrial transfer is currently under discussion with partners in the field.
Sub-project 2 — A map for endomyocardial biopsy
Three conditions — cardiac sarcoidosis, chronic myocarditis and arrhythmogenic cardiomyopathy — can present a similar clinical picture yet call for opposite treatments. To decide, a biopsy is needed… provided the sample is taken in the right place.
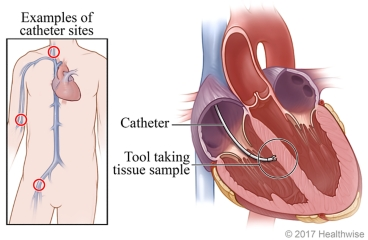
Endomyocardial biopsy: sampling a piece of cardiac tissue, where the lesion is located.
The state of the art leaves a real gap:
- “blind” biopsy is poorly specific, because the fibrosis to target stays invisible during the gesture;
- electro-anatomical guidance is long and, likewise, blind to fibrosis.
Our solution acts as a “GPS” for the biopsy catheter: it transfers the target identified on preoperative imaging onto the real-time image, to guide the sampling. Two design choices make it a solution built for adoption: it is hardware-independent (compatible with an existing room) and works on real-time fluoroscopy, with no complex fusion step. It directly reuses the segmentation building block from the first sub-project.
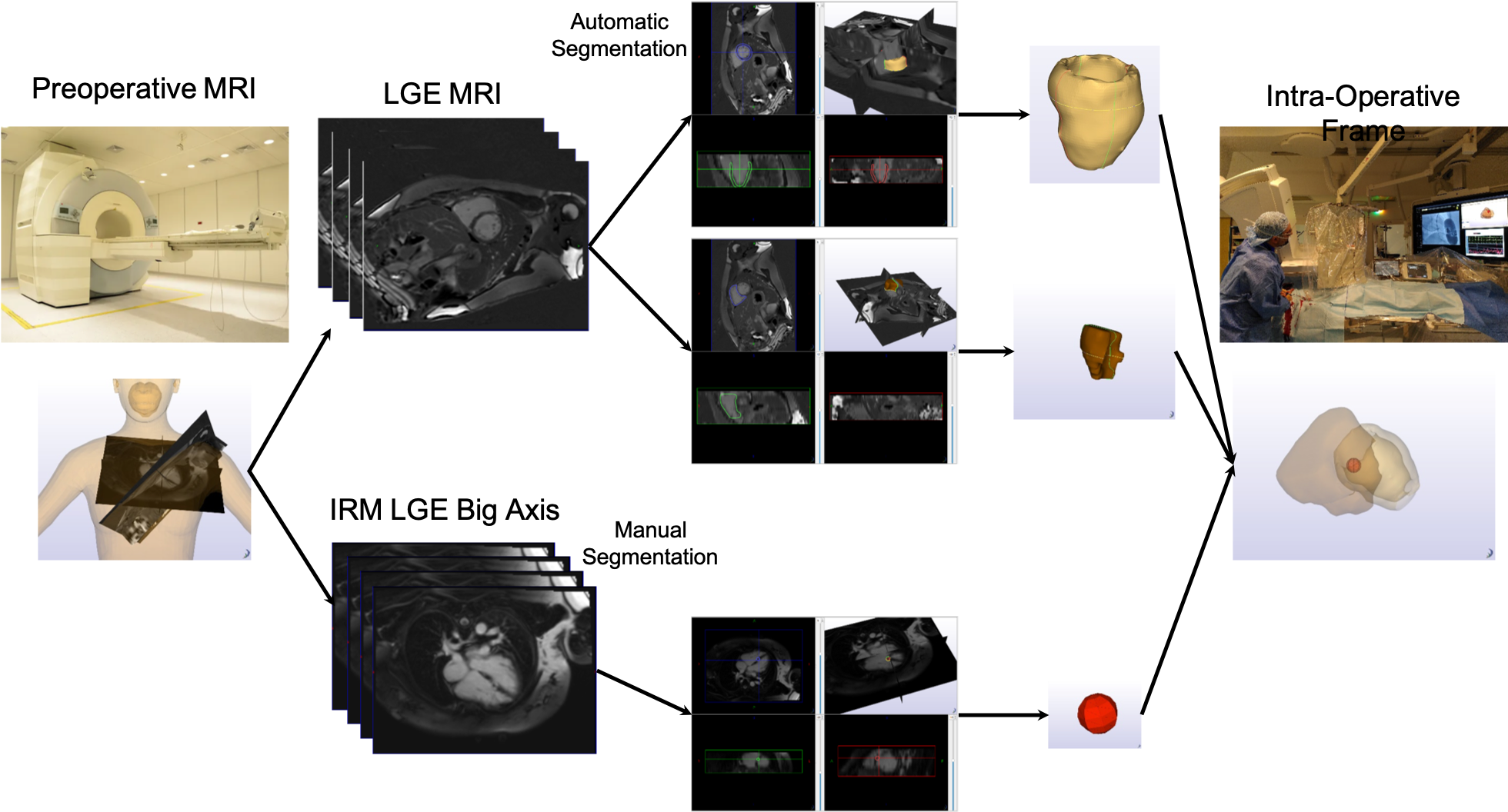
Diagram of the proposed guidance system for endomyocardial biopsy (published).
Current status: we are preparing the first clinical trials in the laboratory; industrial transfer will follow.
What this project demonstrates
- Designing from a real clinical need, in close dialogue with practitioners, rather than around a technical feat.
- Mastering medical image processing and AI, and putting them at the service of a precise, useful target.
- Taking a prototype from the laboratory toward the clinic, with a clear awareness of maturity stages (TRL), the trial framework and CE marking.
- Architecting for adoption: hardware independence, integration into a prototyping toolkit, reuse of building blocks.
- Refocusing a project to preserve its value: agility and de-risking in the face of the unexpected.
- Leading a multi-site collaboration (Grenoble–Rennes) and co-supervising a PhD.
Funding obtained
| Funding | Amount | Purpose |
|---|---|---|
| Famtastic project (France Life Imaging) | €20,000 | Kick-starting the collaboration with the LTSI (Rennes) |
| PUI (UGA) | €60,000 | Maturing the prototype toward the first clinical trials |
| PhD funding (LabeX CAMI) | €170,000 | Co-supervision of Erwan Lecesne’s PhD |
| Post-doctorate (LabeX CAMI) | €56,000 | One year of post-doctoral engineering |
| Total | €306,000 |
Collaborations and supervision
- Prof. Gilles Barone-Rochette — interventional cardiologist, Grenoble Alpes University Hospital: clinical partner of the project.
- LTSI laboratory (Rennes) — Professor Mireille Garreau and Antoine Simon (associate professor): collaboration on cardiac image processing.
- Erwan Lecesne’s PhD (2020–2024), co-supervised at 50% with Mireille Garreau (LTSI): multimodal image processing to improve post-infarction cell therapy.
- Théophile Tiffet’s PhD — medical resident: echocardiography / SPECT calibration for interventional cardiology.
Related publications
- 2024. Barone-Rochette Gilles, MD,, Erwan Lecesne, MSc,, Antoine Simon, PhD, Mireille Garreau, PhD,, Celine Fouard, PhD — New Method CMR-Guided Endomyocardial Biopsy in Suspicion Context of Isolated Cardiac Sarcoidosis. Circulation: Cardiovascular Imaging, vol 17, no 4
- 2023. Erwan Lecesne, Antoine Simon, Mireille Garreau, Barone-Rochette Gilles, Celine Fouard — Segmentation of cardiac infarction in delayed-enhancement MRI using probability map and transformers-based neural networks. Computer Methods and Programs in Biomedicine, vol 242
- 2023. Lecesne Erwan, Simon Antoine, Garreau Mireille, Barone-Rochette Gilles, Fouard Céline — Transformers-Based Neural Network for Cardiac Infarction Segmentation in Delayed-Enhancement MRI. 2023 IEEE Twelfth International Conference on Image Processing Theory, Tools and Applications (IPTA)
